Timely news and topical multimedia discussion focused on Health Information Technology and its role in improving health care. This blog will be the successor to The REC Blog.
A welcome diversion from the hyperpartisan, nihilistic Asshattery in DC. This is inspiring. I have reached out to these people offering to help in whatever ways I can.
It started with a cab drive and a zinger of a line delivered by a seasoned cabbie. "Welcome to the land of broken dreams," he said. Those seven words, a desire to bring about change, and a belief that mobile/moveable could be powerful set in motion what eventually became Lava Mae. Started by private citizens who believe that access to showers and toilets shouldn't be a luxury, Lava Mae is a nonprofit project that seeks to reach the homeless who lack access to these necessities.
When I first saw this, mentioned in an article in the SF Chronicle, I thought immediately of my friend the heroic Dr. Jan Gurley, a national authority on the medical plight of the homeless.
What the NFL and the Homeless Have in Common May 10th, 2011 With a traumatic brain injury, you feel yourself slipping away. You can’t remember things that used to come easily, things like how to find the grocery store — acts and details that live, mocking, at the edges of your thoughts, just outside your grasp.
You know there’s something wrong, but you have a sense that it’s all your fault. Rage bubbles and pops to the surface, the only emotion that seems to escape the thick stew of depression that dulls your days.
You make lists and lists, trying to get your life under control. But two days later, you stare at pieces of paper, trying to remember what the scribble meant, which thing it is that you were supposed to do next.
Chronic pain is there all the time, and you try to plan and wait and be patient and stick with a process, but then you find yourself sitting, head in hands, unable to remember what’s next. All you know is that something’s wrong. And the rage squirms and writhes, trying to bubble up again.
The behavioral changes and impaired functioning caused by post-traumatic brain injury aren’t poignant science fiction. They’re real.
Traumatic brain injury, especially from repeated concussions, has become a pivotal topic in sport, particularly in the National Football League. Watching a game on TV, it used to be easy to scoff at the concept, as you watched players collide a million times and heard the dull thud of plastic against muscle, bone against bone. You’ve seen players get up and walk it off. How could it be life-damaging? And even if it is, didn’t they kind of ask for it?
Watching these young men with lightning fast reflexes and rippling dunes of muscles – symbols, really, of human perfection – it may be hard to believe that they could have anything in common with the guy elbow-deep in the trashcan on your sidewalk. But when it comes to brain injury, its consequences and our reactions to it, the homeless and NFL players may have more in common than you might think...
...70 percent of the homeless reported their first episode of serious head injury before becoming homeless, suggesting, the authors noted, that “in some cases, traumatic brain injury may be a causal factor that contributes to the onset of homelessness, possibly though cognitive or behavioral sequelae of traumatic brain injury.” What’s more, a study like this may actually have under-represented the degree of injury and impairment associated with head trauma among the homeless, since only those people competent enough to seek services at a soup kitchen or shelter were surveyed.
With so much at stake – the loss of human potential, the damage to our society, the costs of care for these kinds of impairments – you might think that society would take very seriously the prevention of head trauma among the homeless. There is, however, a sense that people on the streets may have brought it on themselves.
Assaults resulting in head trauma are a daily occurrence in life on the streets. A head slammed into a dumpster, a dislocating punch to the jaw, a head laceration that’s been stapled closed: these are so common as to be considered “normal” for the homeless...
This is the toughest of tough stuff.
MEANWHILE, BACK IN THE NATION'S CAPITOL
Looks increasingly at this writing (5:12 PDT) like the Republicans are set to Shower the People with bad checks come Thursday.
Should we descend into Default, I rather doubt that anyone will give a
flip about the Meaningful Use initiative on the other side. We will have poured truckloads of salt into our federal deficit wounds. The Health IT MU gravy train will be over. Far more pressing economic concerns will come to the fore.
___
The walled gardens are withering. The silos are splitting open. Disruptive technologies are shaking the heretofore sleepy status quo in myriad ways. No amount of Entrenchment Ambien will suffice to enable any return to the comfy seven figure healthcare space CEO Snooze.
The Disruption will be -- well -- disruptive. It will be messy. There will be casualties. Many of them richly deserving of their plight.
Things I just witnessed at Health 2.0 2013 in Santa Clara comprise yet another wake-up call for me. A lot to think about.
But first, apropos somewhat of my prior post, back to "disruption" of another sort.
Quixotic Queries Question Quality! At healthcare.gov, the plot thickens. At healthcare.gov, many people are still unable to create accounts, choose from a list of health care plans, and sign up for one. The system is down, or overloaded, or shows perplexing errors... I was, it seems, a bit naive in thinking there were merely two cooks (or two bulb managers) in the kitchen behind healthcare.gov. The number of players is considerably larger than just front-end architects Development Seed and back-end developers CGI Federal, although the government is saying very little about who’s responsible. The Department of Health and Human Services’ Centers for Medicare and Medicaid Services (CMS), which issued the contracts, is keeping mum, referring reporters to the labyrinthine USASpending.gov for information about contractors. (I was not able to obtain any useful information from that site, though it does make healthcare.gov look pretty good in comparison.)
By digging through GAO reports, however, I’ve picked out a handful of key players. One is Booz Allen, the people who brought you Edward Snowden. Despite getting $6 million for “Exchange IT integration support,” they now claim that they “did no IT work themselves.” Maybe Snowden can help us out on this one, though as far as I can tell, Booz Allen does seem to be ancillary to the overall healthcare.gov project.
Then there’s CGI Federal, of course, who got the largest set of contracts, worth $88 million, for “FFE information technology and healthcare.gov,” as well as doing nine state exchanges. Their spokesperson’s statement is a model of buck-passing: “We are spending 24 hours a day, seven days a week working with our client and working with our partners in order to stabilize the enrollment [process] and finish the roll-out of this very complex project.”
But which partners? The most interesting is Quality Software Solutions Inc. (QSSI). Despite the laughable name and inexplicable slogans such as “Quality is a Q word”—hard to argue with, I guess—they’ve been doing health care IT since 1997, and got $55 million for healthcare.gov’s data hub in contracts finalized in January 2012. But then UnitedHealth Group purchased QSSI in September 2012, raising eyebrows about conflicts of interest.
In Congressional testimony on Sept. 10, QSSI vice president Michael Finkel said that there was no need to be worried about the conflict of interest—but he also revealed more about the architecture of healthcare.gov and the data hub than anyone else has in the last week. Finkel described the data hub as the ultimate middleman of the entire system, “funneling” queries to databases from multiple sources. This would not be an impossible task, but it would require a formidable level of technical coordination. Imagine if Google, Apple, and Microsoft were suddenly asked to develop a website together...
Development Seed President Eric Gundersen oversaw the part of healthcare.gov that did survive last week: the static front-end Web pages that had nothing to do with the hub. Development Seed was only able to do the work after being hired by contractor Aquilent, who navigated the bureaucracy of government procurement. “If I were to bid on the whole project,” Gundersen told me, “I would need more lawyers and more proposal writers than actual engineers to build the project. Why would I make a company like that?” These convolutions are exactly what prevented the brilliant techies of Obama’s re-election campaign from being involved with the development of healthcare.gov. To get the opportunity to work on arguably the most pivotal website launch in American history, a smart young programmer would have to work for a company mired in bureaucracy and procurement regulations, with a website that looks like it’s from 10 years ago. So much for the efficiency of privatization...
Yikes.
__
SOME QUESTIONS ON THE WAY TO CONVERGENCE
My friend Dr. Andy Pasternak sent me a copy of this to review (BMJ 2013;347 Sept 2013)
With the advent of pay for performance and quality standards, family doctors are now in the business of data reporting. We are paid to report “quality measures” and meet their targets. In the United States, where lawmakers, employers, and patients agree that the cost of healthcare is unsustainable, the government and industry are joining forces to enact structural and payment forms like meaningful use of electronic health records, pay for performance, and the patient centered medical home, which aims to transform the delivery of primary care. These programs reward healthcare providers with new computer systems and added management fees with the expectation of lower costs and measurable improvements in health. But this shift of our gaze to patients’ physiology and chemistry, and to our performance in managing it has unintended consequences. Distracted by data It is reported that physicians spend, on average, 11 minutes with their patients1 and listen to their chief complaint for only 22 seconds before taking control of the interview.2 During these brief encounters, to what or to whom do doctors attend? A structured history of the present illness taken by the medical assistant? The chronic disease flowsheets? A checklist of overdue prevention measures? Doctors have risen to their rank through a fierce competitiveness: we are experts at knowing what to know for the purposes of the test. Increasingly, we are graded on our performance on meeting national guidelines for the control of weight, blood pressure, smoking cessation, cholesterol levels, and diabetes, and the results are reported on consumer websites. It is possible, even likely, that such data will change our approach to patient care. They are already inexorably shaping to what and to whom we listen... The widespread implementation of the electronic health record was intended to reduce the duplication of services, avoid prescribing errors, and increase physicians’ adherence to evidence based guidelines. But it also made it easier to “upcode” encounters with the click of a box. Physicians were often tempted, and sometimes encouraged, to check elements of the history and physical examination that were previously never performed. These failings are obvious when we read our colleagues’ office notes, and now patients aided by online portals are equally aware. The government and other insurers literally pay the price.
Added expense and privacy concerns may be the least of our worries. Computers are peerless at storing, sorting, and reporting data, the kind we gather from laboratory studies and vital signs and checklists. Healthcare payers and the insurance industry use these data to reward and thereby direct the delivery of healthcare according to what is most easily measured. Even Luddites and sentimentalists must acknowledge that medicine cannot, should not, go back to the paper chart. Measurement is a good and necessary thing when it fosters socially responsible research and provides a reality check for human intuition, assumption, and self delusion. But it is never a neutral thing. What we measure unmistakably matters more than what we don’t. And in the age of pay for performance, it speaks to us in the form of incentives that cannot be ignored by our bosses. Wider determinants of health What is health? Or is that a fair question to ask experts on disease? Wendall Berry refers to health as membership. In other words, health is tied to our sense of connection to community. When disease disrupts the bonds of those connections, or requires that they be broken (as for the addict or victim of domestic violence), the doctor’s job is to ease and facilitate the patient’s transition. We are agents of change, from disease to health, from brokenness to a more connected, responsive, and responsible whole. Imagine for a moment that we could redesign our job and the dataset we utilize. What would it look like if there were no bean counters? Could we enlarge our job description to include serving as custodians for an oral history of wounded lives, or as chemists in the complex and volatile setting of human action and reaction?... Facilitating change A primary care physician’s day is largely spent managing the markers of disease: adjusting medications to lower blood pressure, body mass index, or cholesterol level. Too often, it seems like an exercise of “tinkering at the edges.” But once doctors find themselves powerlessness to “fix” the underlying problem, our role can shift to preparing patients for lasting change. Over the past two decades, William Miller and Stephen Rollnick have revolutionized the way in which healthcare workers perceive their role in behavioral change. They call their approach “motivational interviewing” and see it as a directive, client centered counseling style that encourages patients to change their behavior by exploring and resolving ambivalence. Patients are not blind to the risks of their behavior or the benefits change. They simply find themselves stuck in habits both harmful and rewarding. Miller and Rollnick have identified four therapeutic behaviors that are consistently beneficial in helping patients make lasting change: the expression of empathy; the revelation of discrepancies between patients’ problem behaviors and their stated goals; the ability to roll with resistance to change; and, most importantly, support for self efficacy, when patients believe that change is both necessary and possible... Designing our future ...It is not too late to retool the primary care workshop, to redesign the “product” that patients are clamoring for. Some experimentation has already begun. Practitioners of direct primary care have eliminated the health insurance middlemen by offering annual subscriptions. Patients receive affordable primary care; doctors receive an adequate income and sufficient time to spend with their patients. Eric Topol has pioneered the use of sophisticated diagnostic tools at the primary care bedside, thus eliminating the time and expense of a hospital referral. Dennis McCullough is an advocate for slower paced healthcare for elderly people, whose complex medical and social concerns simply need more time.
No doubt, biomarkers of disease will remain a central focus of the clinical gaze, but human faces are emerging on the periphery, and the voice of “America’s doctor” rings with a new air of authenticity: “I would take us all back a thousand years,” Dr Oz mused in a recent interview, “when our ancestors lived in small villages and there was always a healer in that village and his job wasn’t to give you heart surgery or medication but to help find a safe place for conversation. In all fairness, Dr Oz may not be acquainted with primary care or its village healers. If he was, he might find a safe place for conversation and discover what we are learning about connection, childhood trauma, doctor-patient relationships, and the facilitation of change. If we are to remain the masters of our own creation the electronic health record and its data trove̶doctors must submerge it under our plane of awareness, hardwire it into our daily operations, and fence it from the sacred space we reserve for our patients. Only then can we do what we do best: sit presently with our patients and care for them. And allow them to learn, invest, and lead in their own recovery, and in the renewable health resource that is community.
My takeaway here is equal parts "God's Hotel" ("Slow Medicine") and Messrs Weeds' "Medicine in Denial," buttressed by other elements of converging technologies, e.g., evidence-based medicine flowing from increasingly transparent "big data," coupled with personalized data provided by self-monitoring apps and increasingly inexpensive "Lab On A Chip" devices such as those we have just seen demonstrated at Health 2.0.
But, where will government healthcare policy fit with all of this?
Can Government Play Moneyball? How a new era of fiscal scarcity could make Washington work better JOHN BRIDGELAND AND PETER ORSZAGJUN 19 2013, 10:05 PM ET Based on our rough calculations, less than $1 out of every $100 of government spending is backed by even the most basic evidence that the money is being spent wisely. As former officials in the administrations of Barack Obama (Peter Orszag) and George W. Bush (John Bridgeland), we were flabbergasted by how blindly the federal government spends. In other types of American enterprise, spending decisions are usually quite sophisticated, and are rapidly becoming more so: baseball’s transformation into “moneyball” is one example. But the federal government—where spending decisions are largely based on good intentions, inertia, hunches, partisan politics, and personal relationships—has missed this wave.
Allow us to share some behind-the-scenes illustrations of what our crazy system of budgeting looks like—and to propose how the lessons of moneyball could make our government better.
When one of us (Peter) began his tenure as the director of the Congressional Budget Office in 2007, he took a Willie Sutton approach to the nation’s huge and growing fiscal mess: he went after health care, which makes up roughly a quarter of the federal government’s spending, because that’s where the money is. The moneyball formula in baseball—replacing scouts’ traditional beliefs and biases about players with data-intensive studies of what skills actually contribute most to winning—is just as applicable to the battle against out-of-control health-care costs. According to the Institute of Medicine, more than half of treatments provided to patients lack clear evidence that they’re effective. If we could stop ineffective treatments, and swap out expensive treatments for ones that are less expensive but just as effective, we would achieve better outcomes for patients and save money.
Both parties should find much to like in such an approach. It would offer Republicans a way to constrain the growth of government spending and take pressure off private businesses weighed down with health expenses. And it would offer Democrats a means of preserving the integrity of Medicare and Medicaid and thereby restoring faith in a core government function.
And yet getting funding for the research needed to assess and compare medical treatments has been like pulling teeth. As a rule, legislators seem to lack a natural affinity for economists and budget analysts (alas, they are hardly alone). But Peter made himself exceptionally unpopular with some Democrats and many Republicans by insisting on such funding in the 2009 stimulus bill, and then working to expand it in the 2010 “Obamacare” legislation. Despite these modest successes, less than $1 out of every $1,000 that the government spends on health care this year will go toward evaluating whether the other $999-plus actually works.
Getting the right information is less than half the battle. Acting on it, once it’s in hand, is harder still. As one small example, some evidence suggests that moving toward “bundled” payments for all services needed by a patient during a course of medical treatment could produce better value than paying piecemeal for each service and procedure, because the piecemeal approach creates an incentive for more care rather than better care...
It is indisputable, however, that a move toward payments based on performance would harm some business interests. If most of your profits come from, say, a medical device or procedure that is covered by Medicare but doesn’t work all that well, you’re likely to resist anyone sorting through what works and what doesn’t, never mind changing payment accordingly. Health-care interests are wise to invest millions of dollars in campaign contributions and lobbying to protect billions of dollars in profits...
Interesting article. Another problem with "getting the right
information" goes to the partisan politicization of quantitative
findings. Even empirical conclusions of utter scientific rectitude get
battered or summarily dismissed by those with powerful vested interests.
Fundamental to "Lean" process improvement (a.k.a. experimental
scientific method 101) is the outset statement of the problem to be
solved or condition to be improved, the methods to be employed, and the
operational definition of what will constitute an interventional
"success" or statistically "significant" improvement. See Dr.
Toussaint's "On The Mend."
Outset.
You don't decide arbitrarily after the fact on whether you're doing OK.
This appears to be largely lost on government policy and program
planners. Not to say that quantitative after-action review is of no
value, but operational definitions of "success" are better baked in during the program planning phase.___
Notwithstanding the federal shutdown and impasse, the much ballyhoo'ed launch of the PPACA Health Insurance Exchanges went off as scheduled on October 1st while we were at Health 2.0 2013 in Santa Clara.
I spent a bit of time last night surfing around the "Covered California" HIX website.
There will be a lot of unhappy "young invincibles," young, health adults who continue to think they don't need health insurance. After visiting these HIX sites, they will likely not be pleased at what they find -- a lot of "sticker shock" (policy pricetags) and "benefits shock" (out-of-pocket stuff: exclusions, deductibles, and co-pays). Those of us who don't get health insurance through our employers are henceforth to be Individually Mandated Bronze, Silver, Gold, or Platinum people.
Let's look at some Bronze and Silver scenarios for a 30 year old single male earning $40k a year.
Look just at the cheapest Bronze (the Kaiser HMO plan). This fellow will have to fork over $2,784 a year just for the policy (sticker shock), and will then be on the hook for virtually all routine medical expenses up to the out-of-pocket cap (benefits shock -- or, more precisely, "lack-of-benefits shock").
The only year-over year-benefit here is the actual "insurance" piece -- i.e., the "catastrophic" coverage part. The rest is not "insurance," it's "pre-payment" for services that may not be needed for years (in after-tax dollars, I might add). Also, say our $40k earner really only takes home $32k after all deductions. The $6,350 out-of-pocket cap would be ~20% of take-home. Reasonable?
It should be noted that if this hypothetical young man is only making, say, $20k per year, federal subsidies would apply to offset these retail policy prices.
In the foregoing example, assuming no UTIL over the year, the $2,784 (subsidy offsets or not) is essentially a de facto "tax," one not paid into the U.S. Treasury but paid to private health insurance companies.
If the Young Invincibles refuse en masse to jump into the ObamaCare risk pool, the PPACA will simply not work. You're asking young workers to purchase an expensive abstraction. You can touch and feel and watch a top-of-the-line 72" plasma HDTV. You can ride on a nice motorcycle, or ride in a nice power boat. You can take a pretty nice foreign vacation for three grand. A health care "policy," something that you don't want to have to use (and won't if you remain healthy), is quite another matter psychologically.
Jardinero1 says: I accept your feelings about the ACA, Ted Cruz and the ACA but the exchanges are not “the most pro-market thing to emerge from this administration.” They do not fit the definition of markets. Markets are where willing sellers and willing buyers meet without coercion. In the absence of coercion, willing sellers and willing buyers agree on the quality of the good and the price or they agree to walk away from one another. The ACA’s health Insurance exchanges have none of those features. Health insurance exchanges are a state created medium where coerced buyers are forced to buy a product assembled via government edict from a cartel of sellers established by government edict. You could be partially correct if you assert that the state mandated exchange have elements of fascism, state capitalism, or crony capitalism. But call it market based and you are almost wholly incorrect. By coercion, I refer to the threat of violence, loss of freedom (incarceration), or involuntary loss of property (extortion, taxes, fines) under pain of violence or the loss of freedom. Coercion is unique to state mandated activities and organized crime. Free markets are about willing buyers and willing sellers. Forcing people into a room and telling them they have to deal or face the coercion I describe is not a market and not even a market principle.
...Ultimately the fantasy-laden vision that has developed is that capitalism as represented by loosely regulated or unregulated markets is an autonomous, self-stabilizing system that at the same time paradoxically is fragile and mercurial enough to require political and economic “courtship” and “soothing” by local, regional and national governments. Furthermore, this system of economic beliefs suggests that market institutions could do the job of government better than government itself, so it always makes sense for policymakers to try to create markets where there are now government institutions. The fantasy presented is that government is an entirely fallible institution and markets are a nearly infallible institution. If this delusion is assumed as a given, as has been hammered into people’s brains for three decades, logically it makes sense to pare government as much as possible and allow the private sector to attempt to take over its functions...
Obama sold voters bill of goods on health care Debra J. Saunders
As a candidate for president, Barack Obama sold his signature universal health care plan with the promise that it would "cut the cost of a typical family's premium by up to $2,500 a year."
Now that the Affordable Care Act exchanges are open for business, voters are finding that the biggest problem with Obamacare isn't that some Web sites crashed last week but that the Obama promise of big savings for the average family was too good to be true.
Now that the exchanges are open for business, people who already have individual coverage have something new to not like: sticker shock. The Affordable Care Act isn't affordable after all.
Last week, I began hearing from readers whose individual policy premiums are going up, not down. A local architect sent me a notice he received from Kaiser informing him that his individual coverage will increase by $199.95 per month, or 78.9 percent. When he added his two sons, the percentage increase was even greater.
A freelance journalist told me she made $98,000 last year. But she and her retired husband, both 51, wouldn't pay $7,200 in premiums for high-deductible coverage. It's cheaper to pay the fine, she said. Besides, she added, "we're healthy."...
Whether these anecdotes comprise a significant empirical trend or not, it doesn't take more than a relative handful of such stories to turn people off.
__
None of any of the foregoing has anything directly to do with Health IT, of course, but these various pieces of the U.S. health care "system" are increasingly intertwined. Broad support for the PPACA was palpable at Health 2.0 this past week. There's a lot riding on its success.
SNL GOES OFF THE HOOK ON THE SHUTDOWN
Lordy...
The proactive Miley Cyrus parodied her viral song "We Can't Stop" and mocked the U.S. government shutdown on Saturday Night Live. In the pre-taped music video titled "We Did Stop (The Government)," the 20-year-old pop star played congresswoman Michele Bachmann as funny man Taran Killam assumed the role of House Speaker John Boehner.
"It’s our party, we can stop what we want, we can vote how we want, defund what we want," Cyrus sings. "Red states and sweaty bodies everywhere, bill’s in the house like we don’t care, 'cause we came to shut it all down now, no government around now. If you’re not ready for health care, can I get a “hell no!” 'Cause we’re gonna keep it out shut down, D.C.is a closed town all around."
"...Clearly, the usability of EHRs has gotten worse with the implementation of Meaningful Use. Many have been coded to certification requirements, not designed to make achieving Meaningful Use a byproduct of improved workflow automation. Where basic EHR usage is not already established, bolted on functionality forces clinicians to take additional steps that further disrupt workflow..."
Went to an ASQ Section 618 meeting last night in Oakland. Met a lot of very nice people. I'll be switching my Section membership from Las Vegas 705 to the East Bay Section forthwith. I have to get back into being more active in the Society.
Doctors cautious about HIX, says MGMA 40 percent of responding physician practices say they're still weighing their options Diana Manos, October 7, 2013 ...A week into the open enrollment period for ACA insurance exchanges, 40 percent of responding physician practices reported that they are still weighing their options as to whether or not they will participate with new exchange insurance products... "Medical group practices want to continue to do the right thing and take care of patients, regardless of insurance. It’s troublesome that there is so much uncertainty about ACA implementation this late in the game," said Susan L. Turney, MD, MGMA president and CEO in a news release. "Some insurers want practices to sign contracts for less than their current commercial rates, but are unable or unwilling to provide detailed information to physicians about how the exchange products will be administered."...
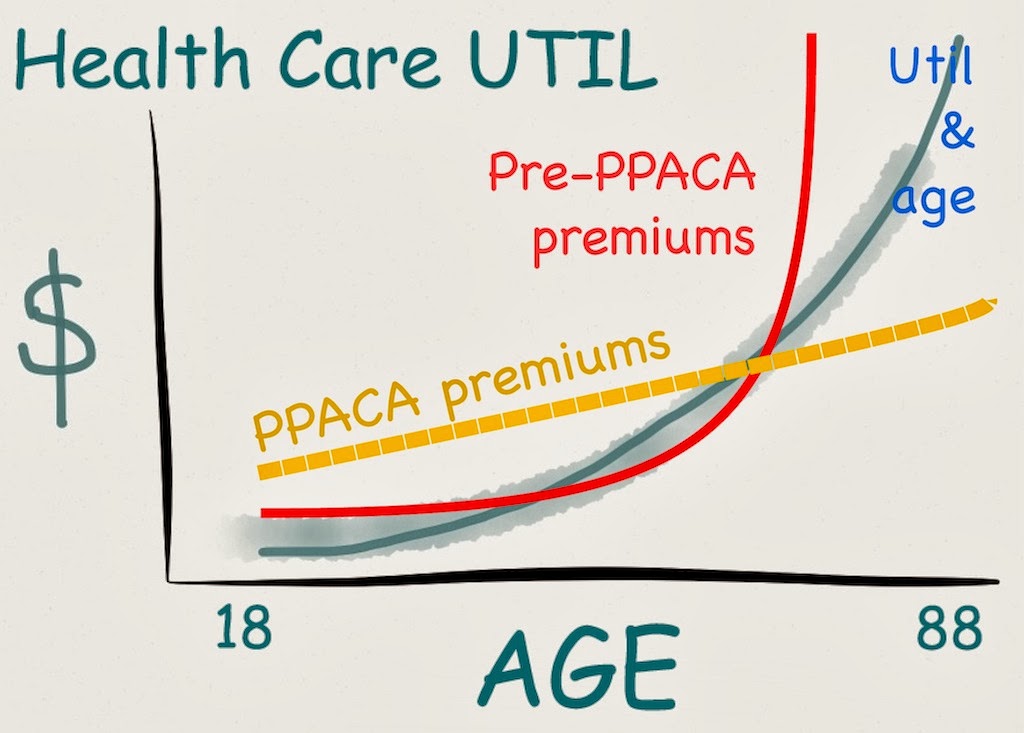
PPACA IN ONE MARKED UP GRAPH
I did a quick Photoshop on the above. On average, health care utilization is a function of aging. We know this, and have known it for a long time. "ObamaCare" is nothing more than a broad redistributional flattening (orange line) of the heretofore prevalent health insurance underwriting model (the red line). The actual "actuarial risk envelope" is 60-70 (adult) years, not one. Once you advance to middle age, you've started costing the insurors money, which they have historically tried to make up by raising rates on the aging, or finding reasons ("pre-existing conditions") to exclude them.
So, yes, the "young have to subsidize the old" in any rational system. But those young will themselves advance to old age, to be reciprocally "subsidized" by the young who follow them. Absent such a payment scheme, the old (with the exception of the very wealthy) will be priced out. No insuror wants to underwrite Grandma.
That's pretty much all there is comprising the topic of this huge political fight now at the center of the acrimonious, paralyzing federal shutdown and looming risk of debt default.
Yes, there are QI pilots contained in the PPACA intended to "bend the UTIL cost curve" down, and advances in medtech such as I just witnessed at Health 2.0 2013 may well abate some costs materially. But, "ObamaCare" is really just insurance reform -- reform that the AHIP members themselves bought into.
CODA
Reposting my ObamaCare song, penned in the wake of the SCOTUS ruling last year.
Monday morning Farzad gave me the nicest compliment I've ever had:
"I
see all these comments on the blogs all the time with trolls bashing
health IT, and you are often the only voice of reason, pushing back
forcefully with facts and logic."
The final day of Health 2.0 2013 was off the hook. Matthew and Indu are
amazing. The entire roster of presenters was amazing. The staff and
volunteers were amazing. The A/V tech crew was amazing. The food was great (but the far-out, groovy, healthy
rice milk and soy milk and no-fat/low-fat milk -- seriously? seriously? I'm with Matthew on that issue. Note to self; bring your own next year).
The receptions were great. My wariness regarding "Big Data" has been materially abated. My jaw is sore from repeatedly dropping to the floor over the Nokia Sensing xChallenge winners. "Disruptive," indeed. Sell your Quest and LabCorp stock (cut your losses) or short them (make money on their demise).
The youngsters presented as "Rising Stars" make me feel old and slow. Scary smart 23- and 24 year old CEOs. Where the hell did I put my hemi-walker and Metamucil?
Fred Trotter is scary smart. Love the new haircut, too, bro.
I want one of those OM Signal body biometrics shirts. Like, today. Where do I send the check?
My skepticism with respect to "employee wellness programs and apps," though, has only hardened. As I commented on September 24th on THCB:
Interesting post. Tomorrow I have to get up early and submit to some “Wellness Screening” stuff at my wife’s company, so that we get some “rate discount.” Having retired from my REC gig, I’m now on her insurance. Just gonna smile, play ball, and not make any waves for now, I guess. I would speculate that, were we able to do a sound scientific study, we’d find that MOST U.S. companies are organizationally/psychodynamically toxic, places where one speaks truth to power at one’s peril (notwithstanding all the cherubic blather about “openness” and “safe culture”), places where backstabbing org chart climbing are rife, places where the bookshelves groan under the weight of books on “leadership” and “empowerment” and “team building.” That, sadly, would characterize my last place of employment — a QIO, REC, and now HIE (for whom I worked 3 times spanning 20 years, noting an accelerating change for the worse). It was a factor in my “retirement” in April. They’d started into this lame HR-driven “wellness” “Re-Education Camp” initiative this year that was pure Dilbert Zone. I pretty much ignored it. Wallpapering pretty “wellness” laminate over toxic business cultures is gonna do little more than decrease operating margins. I’ve worked for seven employers across my white collar career. Only two of them could be considered culturally non-toxic.
Other stuff: A huge, irritating disappointment; the cancellation of the Health 2.0 ONC Town Hall owing to the absurd federal government shutdown. Farzard and his people had to return to DC Monday night.
Another irritant: endless barrages of "This data," "that data," "the data is" (I know; the "data are" battle is largely lost). And, everything is now "curated."
I'm back home, to the delight of my dogs. Fresh half and half in the fridge. Hundreds of photos to review and triage, much narrative commentary to ponder and write up. Bear with me. This may take a couple of days to fully reflect upon.
__
FINAL DAY PHOTOS
I will eventually get names affixed to most of these faces (I hope; the action was intense and fast-moving).
Francois de Brantes of Health Care Incentives Improvement Institute
Fred Trotter and his data visualizations
Evolent CEO Frank Williams
Alere's Helen Figge
Dignity Health CEO Lloyd Dean
Todd Rothenhaus, AthenaHealth
Adam Perer on big data complex patient clinical outcomes mapping
This interative node/path stuff reminds me of the kind of CART analytics stuff I used to do in banking (pdf). e.g., below:
Above: the fabulous Epocrates "Bugs and Drugs" smartphone app
Yeah, what if your smartphone could warn you of an incipient stroke?







































































{kind=link}